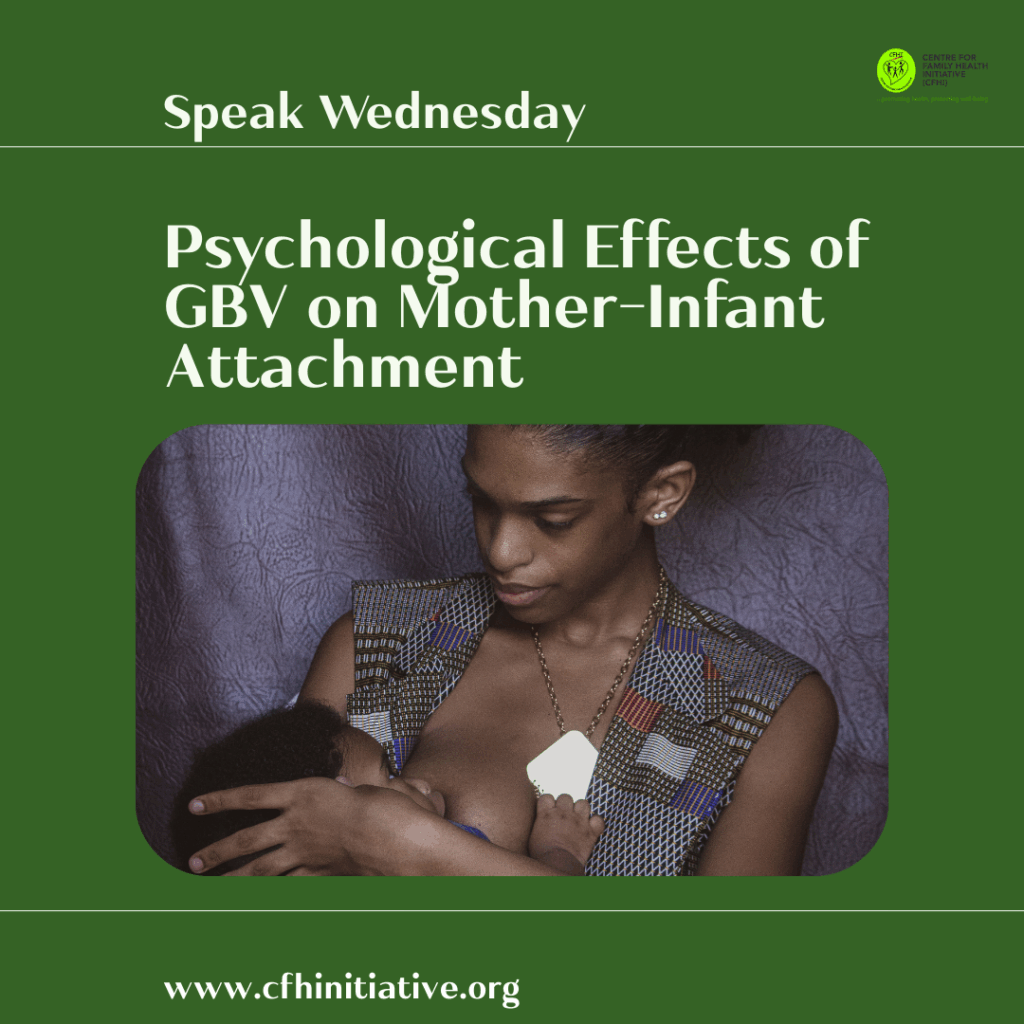
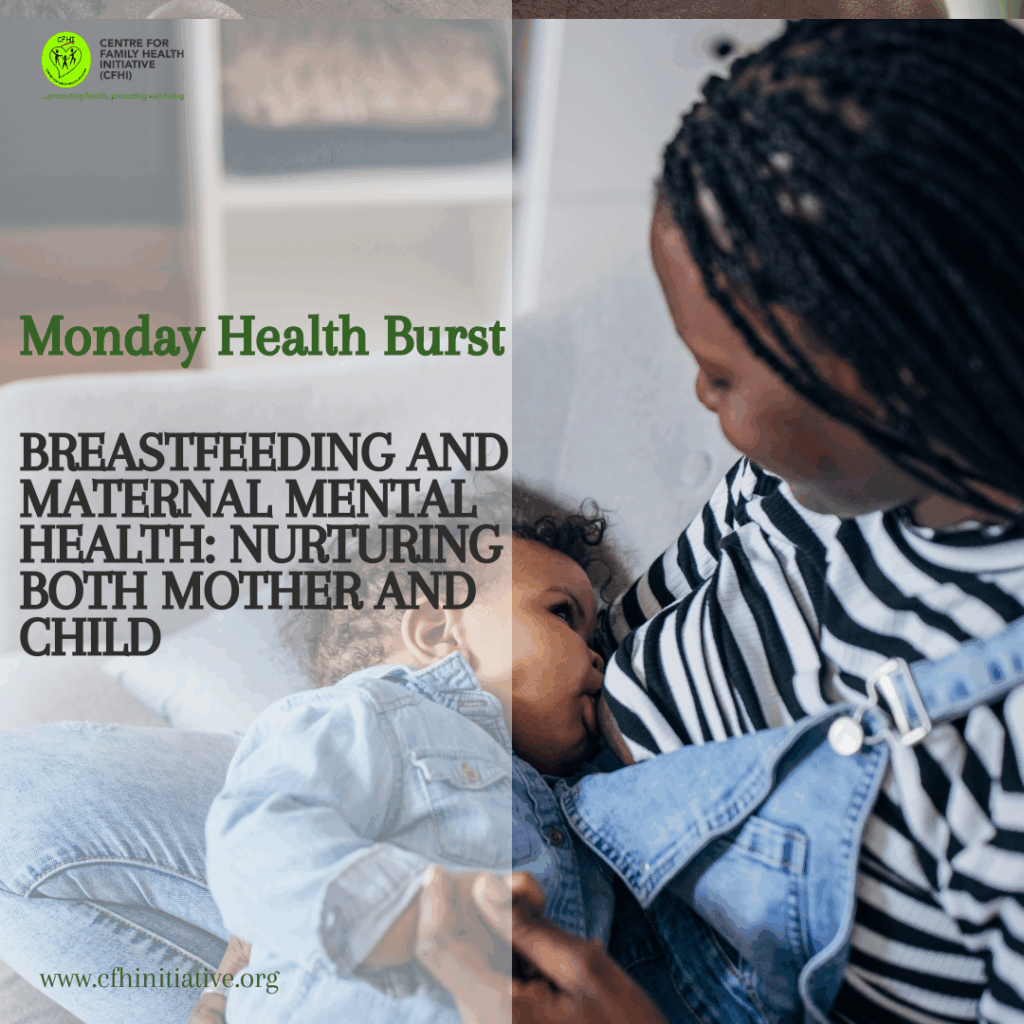
“You can’t nourish from an empty cup, and you definitely can’t breastfeed through trauma.”
The right to nourishment is a fundamental human right. Yet, for millions of infants in Nigeria and around the world, that right is compromised from birth, not by poverty alone, but by violence inflicted on the very individuals tasked with nurturing them. As the world marks World Breastfeeding Week, it is imperative to confront a rarely addressed but devastating intersection: the relationship between gender-based violence (GBV) and infant health, particularly breastfeeding outcomes.
Breastfeeding is globally recognized as a cornerstone of infant survival and development. According to the World Health Organization (WHO), optimal breastfeeding could prevent over 823,000 child deaths annually across the globe. However, in households where women face psychological, physical, or sexual violence, the act of breastfeeding becomes compromised, interrupted, or entirely abandoned, placing infants at heightened risk of disease, malnutrition, and death.
Understanding Gender-Based Violence in Nigeria
In Nigeria, gender-based violence is a pervasive issue. According to the National Demographic and Health Survey (NDHS), 30% of Nigerian women aged 15–49 have experienced physical violence since age 15, and 9% experienced sexual violence. The figures are even higher in certain rural communities and internally displaced persons (IDP) camps, where systemic poverty, displacement, and insecurity magnify the risks.
This violence is not limited to isolated acts of cruelty. It is embedded in socio-cultural systems that normalize women’s suffering and silence, even during vulnerable periods such as pregnancy and postpartum. These environments profoundly impact maternal mental health and consequently, infant care practices.
How Gender-Based Violence Impacts Breastfeeding
Numerous peer-reviewed studies affirm that women who experience GBV, especially during or immediately after pregnancy, are significantly less likely to initiate or continue breastfeeding.
1. Physiological Disruption of Lactation
The stress caused by violence increases cortisol levels, which can inhibit the production of oxytocin, a hormone essential for milk let-down. In essence, a mother’s body under chronic threat cannot perform its nurturing functions efficiently.
2. Mental Health Consequences
Women exposed to intimate partner violence (IPV) are at increased risk of postpartum depression, anxiety, and post-traumatic stress disorder (PTSD). These conditions are linked to early cessation of exclusive breastfeeding.
3. Limited Access to Healthcare
GBV survivors are often restricted in their mobility and decision-making, making them less likely to access maternal health services. This further reduces opportunities for lactation counseling or timely postnatal care, which are vital for breastfeeding success.
4. Physical Trauma
Injuries to the breasts or upper body from physical abuse can make breastfeeding painful or physically impossible. Moreover, repeated violence erodes a mother’s sense of bodily autonomy, which may deter her from engaging in breastfeeding altogether.
Impact on Infant Health
When mothers are unable to breastfeed exclusively for the first six months, a practice strongly endorsed by WHO and UNICEF, the consequences for infants are profound:
• Increased risk of diarrhea, respiratory infections, and undernutrition.
• Higher likelihood of stunted growth and developmental delays.
• Elevated infant mortality, particularly in settings with limited access to safe alternatives.
In Nigeria, where 44% of children under five are stunted, the added burden of disrupted breastfeeding due to GBV further deepens a national child health crisis.
Sociocultural and Structural Drivers
In many Nigerian communities, cultural norms that promote male dominance and female submissiveness inhibit women’s ability to seek help or resist abuse. Violence is often dismissed as “discipline” or a private family affair. These norms are reinforced by:
• Patriarchal interpretations of religion
• Bride price systems that commodify women
• The stigmatization of divorced or single mothers
• Poor legal enforcement of existing protective laws, such as the Violence Against Persons (Prohibition) Act (VAPP Act) of 2015, which remains unadopted in several Nigerian states.
As a result, maternal silence becomes survival, even when that silence compromises infant health.
Recommendations: Multisectoral Action is Imperative
Addressing the impact of GBV on breastfeeding and infant health requires coordinated efforts across health, legal, and community systems. The following actions are recommended:
1. Integrate GBV Screening into Maternal and Child Health Services
Health workers at antenatal, delivery, and postnatal care points must be trained to screen for and respond to GBV sensitively and confidentially.
2. Strengthen Legal Protection and Enforcement
Full domestication and enforcement of the VAPP Act in all 36 states is non-negotiable. Legal systems must prioritize survivor protection, not the preservation of abusive family structures.
3. Community Education and Norms Change
Religious and traditional leaders must be engaged as advocates for safe motherhood. Community dialogues can play a key role in dismantling harmful gender norms.
4. Expand Access to Psychosocial Support
Psychological care, trauma counseling, and peer-support networks for survivors should be embedded within maternal health programs.
5. Data Collection and Research
More localized data is needed to map the intersection of GBV and breastfeeding outcomes in Nigeria. Without robust data, interventions risk being misaligned or underfunded.
Conclusion
Breastfeeding is not only a health practice; it is an act of nurturing, safety, and trust. When a mother is forced to feed through fear, we undermine not just her health but the health of the next generation. Ending GBV is not a side issue in public health; it is central to child survival, gender equity, and national development.
This week, as we celebrate World Breastfeeding Week, we must reaffirm that the ability of Nigerian women to breastfeed in safety and dignity is a national imperative. Silence and cultural complicity can no longer be tolerated. The future of our children, indeed, of our nation, depends on it.
Speak Wednesday is an initiative of CFHI to address issues around gender-based violence and gender bias.
#WorldBreastfeedingWeek #EndGBV #InfantHealth #MaternalHealth #BreastfeedingMatters #SafeMotherhood #SupportSurvivors #NutritionJustice #HealthEquity #VAPPAct #WomensRights
References
• World Health Organization (2017). Protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services. https://www.who.int
• National Population Commission (NPC) [Nigeria] and ICF. (2019). Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, USA.
• UNICEF (2019). Programming Guidance: Infant and Young Child Feeding in Emergencies. https://www.unicef.org
• Kendall-Tackett, K. A. (2007). Violence against women and the perinatal period: The impact of lifetime violence and abuse on pregnancy, birth, and breastfeeding. Trauma, Violence, & Abuse, 8(3), 344–353.
• Silverman, J.G., Decker, M.R., Reed, E., & Raj, A. (2006). Intimate partner violence around the time of pregnancy: Association with breastfeeding behavior. Journal of Women’s Health, 15(8), 934–940.
• Kumar, M., Huang, K., Othman, S., Rahman, M., & Lee, S. (2017). Effect of intimate partner violence on breastfeeding behavior: A systematic review. BMJ Open, 7:e014439.
• UNHCR (2021). Nigeria Factsheet – Gender-Based Violence. https://www.unhcr.org/ng
• World Health Organization (2021). Infant and Young Child Feeding. https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding