Beyond Stigma: Community-Led Support for Women and Girls Living with HIV
Stigma remains one of the greatest obstacles to ending HIV: globally, according to the latest UNAIDS estimates, about 40.8 million people were living with HIV as of the end of 2024, with women and girls accounting for approximately 53% of all infections [1]. Despite progress in expanding treatment access bringing lifesaving antiretroviral therapy to over 31 million people worldwide millions still face stigma, discrimination, and social exclusion, which continue to limit their ability to seek testing, care, and long-term support [1].
Evidence shows that stigma discourages people from testing, delays linkage to treatment, and undermines adherence; pooled analyses across African surveys and facility studies find that people who experience stigma are significantly less likely to know their status or remain engaged in care, which in turn reduces chances of viral suppression and worsens health outcomes [2,3]. The scientific consensus that “U=U” (Undetectable = Untransmittable) underscores why ending stigma is also a prevention strategy: people on effective antiretroviral therapy (ART) who achieve and maintain an undetectable viral load do not sexually transmit HIV [4]. Despite these advances, gaps remain UNAIDS reports that while millions are on treatment, about 31.6 million people were accessing ART in 2024, leaving a substantial number still unreached by life-saving services [1].
Community-led support is central to bridging those gaps for women and girls. Practical, evidence-based community interventions peer support groups, community health worker follow-up, safe disclosure spaces, integrated mental-health services, and targeted outreach to adolescents have been shown to increase testing uptake, improve retention on ART, and reduce internalized stigma [5,6]. In Nigeria and other countries, facility-level and community studies link stigma with lower adherence and higher loss to follow up, highlighting the need for local, culturally sensitive responses that engage families, faith leaders, youth networks, and women’s groups [3,7]. Gender-sensitive programming is particularly important: women and girls face intersectional stigma driven by gender norms, economic dependence, and the risk of gender-based violence barriers that require combined social protection, livelihood support, and confidential clinical services to overcome [5].
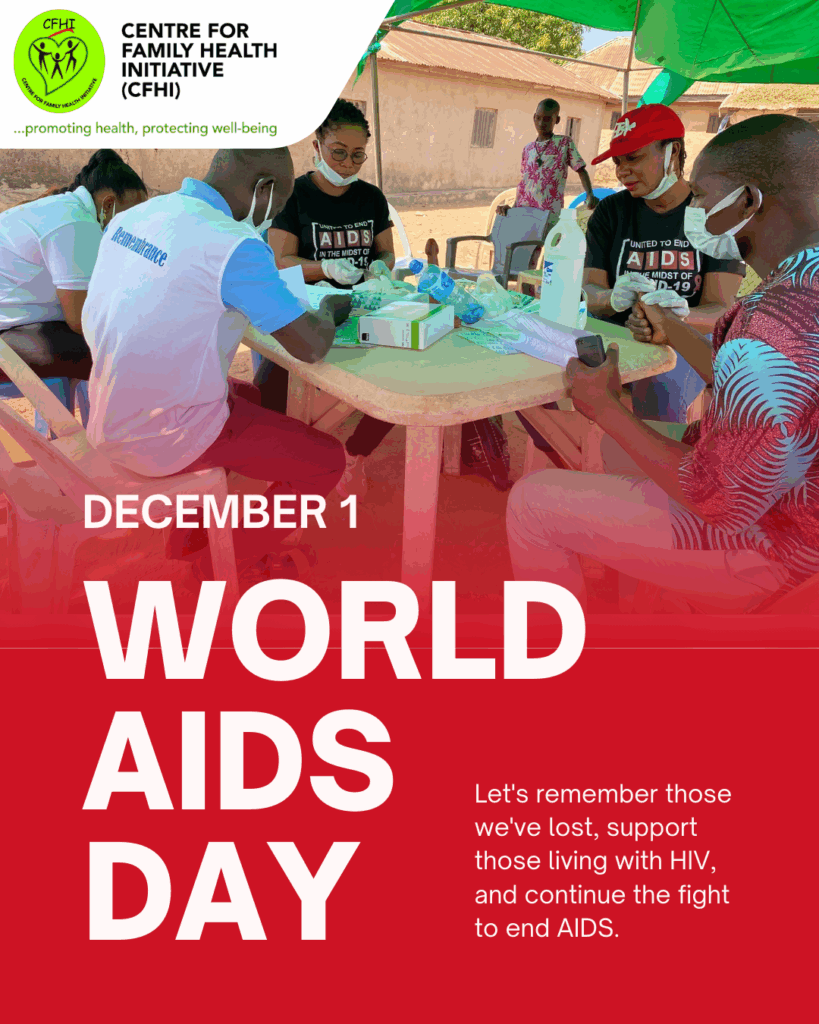
At the Centre for Family Health Initiative (CFHI), community-led support is operationalized through sustained activities that go beyond one-day events. CFHI provides community HIV testing and counselling, adolescent-friendly education, psychosocial support, and peer navigation to link women and girls to care and keep them on treatment [8]. The organization integrates stigma-reduction messaging into gender-norms dialogues, trains community health volunteers in respectful care, and runs livelihood and empowerment sessions that reduce economic vulnerability an important factor that often forces women to remain in situations where disclosure is dangerous. CFHI’s community outreach also emphasizes U=U messaging to demystify treatment and encourage adherence and last year’s community testing and sensitization activities in Imo State reached hundreds with counselling and referrals, reinforcing the role of sustained local engagement in improving outcomes [8].
Ending HIV stigma requires action across sectors. Health facilities must adopt anti-discrimination policies and provide confidential, quality services; community leaders and faith institutions must publicly reject harmful narratives; schools and youth groups must deliver age-appropriate HIV education; and social protection programmes should prioritize women and girls so economic dependence does not block access to care. Donors and governments must sustain funding for community-led responses, which evidence shows are cost-effective and essential for reaching the UN targets to end AIDS as a public health threat [5,6].
Now is the time for communities to move from awareness to durable action. Support people living with HIV by learning and sharing accurate facts, joining, or starting peer support groups, encouraging friends and family to test, demanding respectful care at clinics, and supporting empowerment programmes that reduce vulnerability. CFHI and partners stand ready to work with communities, faith groups, schools, and health services to build safe, supportive environments where women and girls living with HIV can thrive. Together we can make stigma a thing of the past because when communities lead, lives change.
References
- Global HIV & AIDS statistics — Fact sheet. Geneva: Joint United Nations Programme on HIV/AIDS; 2025.
Available from: https://www.unaids.org/en/resources/fact-sheet - Doyle CM, Kuchukhidze S, Stannah J, Flores Anato JL, Xia Y, Logie CH, et al. The impact of HIV stigma and discrimination on HIV testing, antiretroviral treatment, and viral suppression in Africa: a pooled analysis of population-based surveys.
Available from: https://www.researchgate.net/publication/391079137_The_Impact_of_HIV_Stigma_and_Discrimination_on_HIV_Testing_Antiretroviral_Treatment_and_Viral_Suppression_in_Africa_A_Pooled_Analysis_of_Population-Based_Surveys - Mahlalela NB, et al. The association between HIV-related stigma and health-seeking behaviour, testing and adherence: a systematic review. J Public Health. 2024.
Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10896802/ - UNAIDS / IAS / Prevention Access Campaign. Undetectable = Untransmittable (U=U) consensus and evidence. Geneva: UNAIDS; 2018–2024.
Available from: https://www.unaids.org/en/resources/presscentre/featurestories/2018/july/undetectable-untransmittable - World Health Organization. Eliminating stigma and discrimination in HIV responses: evidence and interventions. Geneva: WHO; 2022.
Available from: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics - Community-led monitoring / Community-led responses — evidence and good practice. Geneva: UNAIDS; 2023.
Available from: https://www.unaids.org/en/resources/documents/2023/community-led-monitoring-in-action - Okunola A, et al. The impact of stigma on ART adherence in Ondo State clinics: cross-sectional evidence. Int J Res Innov Social Sci. 2025.
Available from: https://rsisinternational.org/journals/ijriss/articles/the-impact-of-stigma-and-discrimination-on-adherence-levels-in-hiv-positive-patients-evidence-from-ondo-state-clinics/ - Centre for Family Health Initiative (CFHI). Community HIV services, stigma reduction and outreach report. Owerri: CFHI; 2024–2025.
Available from: https://www.cfhinitiative.org
Beyond Stigma: Community-Led Support for Women and Girls Living with HIV Read More »