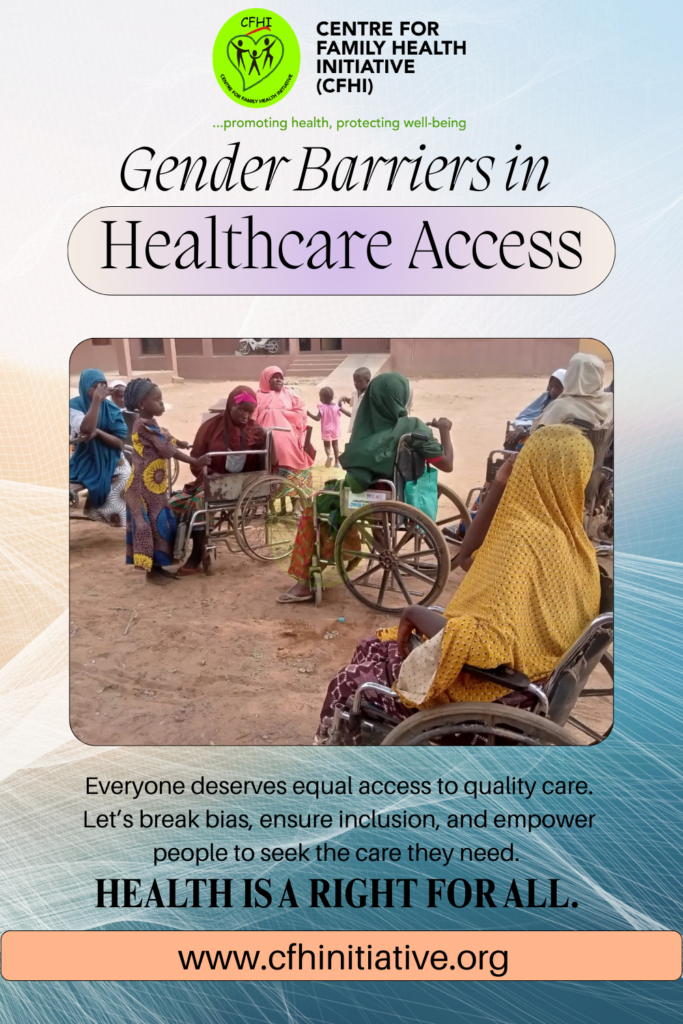
Removing Gender Barriers in Healthcare Access
Removing gender barriers to healthcare is not only a matter of equity it is a moral and practical necessity if societies are to survive and thrive. Women and girls face layered obstacles to care: constrained mobility, financial dependence, harmful social norms, and health systems that are under-resourced and sometimes discriminatory. The World Health Organization highlights that gender norms and discrimination systematically limit access to services for women and girls, reducing their ability to obtain timely information, preventive care, and lifesaving treatment (1). These barriers are compounded by grim facility gaps: recent WHO/UNICEF data show billions are treated in health settings that lack basic water, sanitation, hygiene, and reliable electricity conditions that make safe maternal care and emergency treatment precarious (2). At the same time, progress toward universal health coverage (UHC) has slowed, leaving significant groups especially women in rural and low-income communities exposed to out-of-pocket costs and unmet needs (3).
The consequences are measurable and stark. Nigeria, for example, continues to bear a disproportionate share of global maternal deaths, a reality linked to regional inequalities in access, weak infrastructure, and funding shortfalls (4). Globally, analyses of health inclusivity reveal that refugees, displaced women, women with disabilities and other marginalized groups are far more likely to be denied or excluded from care in some cases by more than twenty percentage points compared with non-marginalized groups (5). These are not abstract injustices: they translate into delayed antenatal visits, unattended deliveries, untreated complications, and endless cycles of preventable suffering. Removing gender barriers means addressing the social drivers that prevent women from seeking care as urgently as fixing the physical gaps in facilities.
Civil society organisations and local actors are essential partners in closing these gaps. The Centre for Family Health Initiative (CFHI) works at the community level to confront both practical and cultural barriers to care: we run health education and rights-awareness campaigns that equip women and families with knowledge about available services and how to claim them; we strengthen linkages between households and primary health centres through referrals and case management; we support WASH and menstrual hygiene programmes so women can access services with dignity; and we provide capacity building for community health workers and facility staff so that care is both accessible and respectful (6). Where infrastructure is missing, CFHI has partnered with donors and initiatives to deliver pragmatic solutions for example installing solar birth kits in underserved PHCs to ensure safe night-time deliveries while simultaneously training Healthcare Professionals and Community Health Extension Workers (CHEWs) to enhance their competencies in clinical care, documentation, counselling, and emergency response, ensuring that PHCs can deliver reliable and respectful services across all essential health areas
To remove gender barriers at scale, governments, donors, and health systems must act on several fronts. First, finance primary health care adequately and ensure that essential services are free or financially protected at the point of use, so women are not forced to choose between care and survival. Second, invest in facility infrastructure WASH, electricity, cold chain and privacy provisions because dignity and safety are prerequisites for access. Third, embed gender-responsive policies across health programming: mandate respectful maternity care, train providers on implicit bias and discrimination, involve women and adolescent girls in service design, and expand targeted outreach for marginalized groups. Fourth, strengthen data systems to capture gender-disaggregated indicators and unmet needs so resource allocation can follow the evidence. Finally, create accountability mechanisms community scorecards, patient charters and independent oversight so promises become measurable action.
Change requires more than policy papers; it requires citizens, health workers, NGOs and governments to demand it and to act. We call on policymakers to prioritise gender responsive UHC financing and facility upgrades, on donors to fund long-term health system strengthening rather than short-term projects, on facility managers to adopt respectful care protocols today, and on community leaders to champion women’s right to health. If we truly value half our population, we will remove the gender barriers that deny women the healthcare they are owed.
References
- World Health Organization. Gender and health. Available from: https://www.who.int/health-topics/gender.
- World Health Organization; UNICEF. Countries making unprecedented efforts but billions still lack basic services in health-care facilities — WHO-UNICEF report warns. WHO website. 24 Sep 2025. Available from: https://www.who.int/news/item/24-09-2025-countries-making-unprecedented-efforts-but-billions-still-lack-basic-services-in-health-care-facilities—who-unicef-new-report-warns.
- World Health Organization. Universal health coverage (UHC) fact sheet. Available from: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc).
- The Guardian. ‘Difficult choices’: aid cuts threaten effort to reduce maternal deaths in Nigeria. 21 May 2025. Available from: https://www.theguardian.com/world/2025/may/21/aid-cuts-threaten-effort-reduce-maternal-deaths-nigeria.
- Economist Impact. Understanding health inclusivity for women. Available from: https://impact.economist.com/projects/health-inclusivity-index/inclusivity-topics/articles/understanding-health-inclusivity-for-women.
- Centre for Family Health Initiative (CFHI). Who we are / What we do. Available from: https://www.cfhinitiative.org.
Removing Gender Barriers in Healthcare Access Read More »