Integrated Health and Sanitation Approaches for Tuberculosis Prevention
Tuberculosis (TB) remains a major public health concern globally and in Nigeria, requiring a comprehensive and integrated approach that combines healthcare services with sanitation and environmental interventions. TB is caused by Mycobacterium tuberculosis and spreads through airborne droplets when an infected person coughs or sneezes. Globally, TB continues to be one of the leading infectious killers, with millions of new infections recorded annually. Nigeria is among the top high-burden TB countries, with an estimated incidence rate of 219 cases per 100,000 population and hundreds of thousands of infections reported yearly². Despite progress, gaps in early detection, treatment access, and environmental health conditions continue to drive transmission.
An integrated approach to TB prevention recognizes that the disease is not only a medical issue but also closely linked to living conditions, sanitation, and social determinants of health. Research shows that TB transmission is higher in overcrowded, poorly ventilated, and unsanitary environments, where airborne bacteria can easily spread⁷. In many communities, poor housing, inadequate waste management, and lack of hygiene practices contribute to increased exposure. Studies further highlight that weak implementation of infection prevention and control measures in health facilities also increases transmission risks among patients and healthcare workers⁷.
Effective TB prevention therefore requires combining health interventions with sanitation and hygiene (WASH) strategies. From a health systems perspective, early diagnosis and prompt treatment are critical. The World Health Organization emphasizes that starting TB treatment quickly after diagnosis significantly reduces transmission and improves outcomes¹. In addition, contact tracing and active case finding have proven effective. For instance, community-based screening interventions in Nigeria have shown that targeted contact investigation yields higher TB detection rates compared to general screening approaches, demonstrating the importance of integrated community health strategies¹².
Sanitation and environmental health measures also play a vital role in TB prevention. Improving ventilation in homes, schools, and health facilities reduces the concentration of infectious droplets in the air. Promoting good hygiene practices, such as covering the mouth when coughing and reducing indoor air pollution, helps limit transmission. Addressing overcrowding and ensuring access to clean and safe living environments are equally important. Furthermore, strengthening nutrition is essential, as malnutrition weakens immunity and increases susceptibility to TB infection.
Integrated interventions must also address vulnerable populations. TB is closely associated with HIV infection, poverty, and weak immune systems, making collaborative TB/HIV programs essential. In Nigeria, about 4.9% of TB patients are co-infected with HIV, highlighting the need for integrated service delivery that includes HIV testing, treatment, and TB care⁰. The global End TB Strategy also emphasizes patient-centered care, strong health systems, and community engagement as key pillars for reducing TB burden⁵.
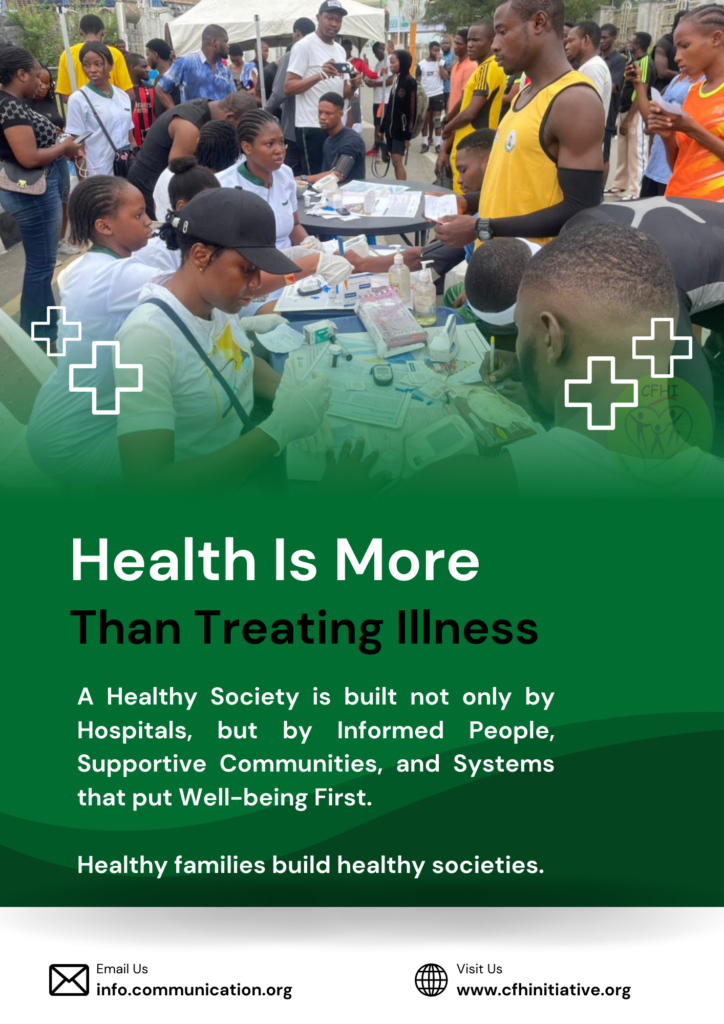
Organizations like the Centre for Family Health Initiative (CFHI) play a critical role in advancing integrated TB prevention efforts in Nigeria. Through community-based programs, CFHI supports TB awareness, screening, referral, and linkage to treatment services, particularly among vulnerable populations such as children, adolescents, and people living with HIV. The organization also promotes health education, hygiene practices, and community mobilization, helping to address both the medical and environmental factors driving TB transmission. CFHI’s work aligns with national and global strategies that emphasize integration of health services with social and behavioral interventions.
To strengthen TB prevention, several measures should be prioritized. First, expand community-based TB screening and early diagnosis services to detect cases early. Second, improve sanitation and housing conditions, especially in high-density communities. Third, promote WASH interventions, including hygiene education and environmental cleanliness. Fourth, strengthen infection prevention and control practices in health facilities to protect both patients and healthcare workers. Fifth, increase public awareness campaigns to reduce stigma and encourage timely healthcare seeking. Finally, ensure consistent access to free TB treatment and adherence support, as treatment success rates can reach over 90% when properly followed⁰.
The fight against tuberculosis requires a multi-sectoral and integrated response that goes beyond clinical treatment. By combining health services with sanitation, environmental improvements, and community engagement, it is possible to significantly reduce TB transmission and improve health outcomes. Individuals also have a role to play by seeking early testing when symptoms appear, maintaining good hygiene practices, and supporting affected persons without stigma.
Tuberculosis is preventable and curable, but only when detected and treated early. Communities, health workers, organizations, and policymakers must work together to strengthen integrated health and sanitation interventions. If you experience symptoms such as a persistent cough lasting more than two weeks, fever, or weight loss, visit the nearest health facility for testing. Together, through improved hygiene, better living conditions, and timely treatment, we can reduce the burden of TB and move closer to ending the epidemic.
References
- World Health Organization – TB Prevention and Infection Control
https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2023/tb-prevention - CDC Nigeria TB Data and Statistics
https://www.cdc.gov/global-hiv-tb/php/where-we-work/nigeria.html - WHO Global Tuberculosis Programme – Nigeria Case Study
https://www.who.int/docs/default-source/documents/tuberculosis/engage-tb-nigeria-case-study.pdf - National Tuberculosis and Leprosy Control Programme (NTBLCP)
https://ntblcp.org.ng/ - WHO End TB Strategy Overview
https://afro.who.int/health-topics/tuberculosis-tb - BMC Public Health – TB Burden and Treatment Outcomes in Nigeria
https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-09289-x - BMC Infectious Diseases – TB Infection Control in Nigeria
https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-016-1453-y - TB Preventive Practices Study (Nigeria)
https://pmc.ncbi.nlm.nih.gov/articles/PMC10262855/ - TB Infection Control Study (Enugu, Nigeria)
https://pmc.ncbi.nlm.nih.gov/articles/PMC9120735/ - WHO TB Case Finding Initiatives in Nigeria
https://www.afro.who.int/countries/nigeria/news/intensifying-new-initiatives-tb-case-finding-nigeria
Integrated Health and Sanitation Approaches for Tuberculosis Prevention Read More »